
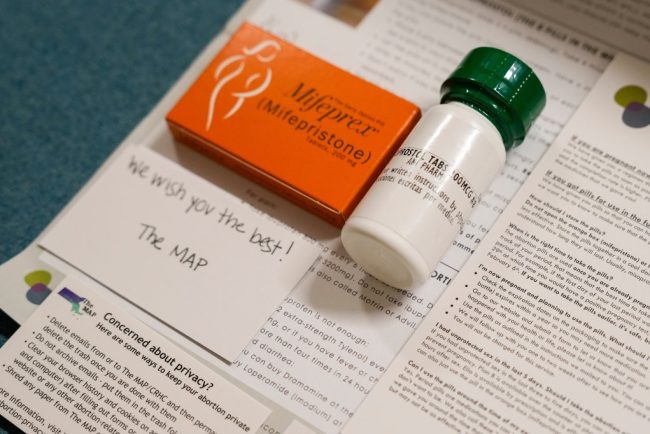
Despite Historic Indictment, Doctors Will Keep Mailing Abortion Pills Across State Lines
When the news broke on Jan. 31 that a New York physician had been indicted for shipping abortion medications to a woman in Louisiana, it stoked fear across the network of doctors and medical clinics who engage in similar work. “It’s scary. It’s frustrating,” said […]
Pharmaceuticals
At Social Security, These Are the Days of the Living Dead
Rennie Glasgow, who has served 15 years at the Social Security Administration, is seeing something new on the job: dead people. They’re not really dead, of course. In four instances over the past few weeks, he told KFF Health News, his Schenectady, New York, office […]
Health Care
HIV Testing and Outreach Falter as Trump Funding Cuts Sweep the South
JACKSON, Miss. — Storm clouds hung low above a community center in Jackson, where pastor Andre Devine invited people inside for lunch. Hoagies with smoked turkey and ham drew the crowd, but several people lingered for free preventive health care: tests for HIV and other […]
Health Care



Covid Worsened Shortages of Doctors and Nurses. Five Years On, Rural Hospitals Still Struggle.
Even by rural hospital standards, Keokuk County Hospital and Clinics in southeastern Iowa is small. The 14-bed hospital, in Sigourney, doesn’t do surgeries or deliver babies. The small 24-hour emergency room is overseen by two full-time doctors. CEO Matt Ives wants to hire a third […]
Rural HealthEven by rural hospital standards, Keokuk County Hospital and Clinics in southeastern Iowa is small.
The 14-bed hospital, in Sigourney, doesn’t do surgeries or deliver babies. The small 24-hour emergency room is overseen by two full-time doctors.
CEO Matt Ives wants to hire a third doctor, but he said finding physicians for a rural area has been challenging since the covid-19 pandemic. He said several physicians at his hospital have retired since the start of the pandemic, and others have decided to stop practicing certain types of care, particularly emergency care.
Another rural hospital is down the road, about a 40-minute drive east. Washington County Hospital and Clinics has 22 beds and is experiencing similar staffing struggles. “Over the course of the last few years, we’ve had not only the pandemic, but we’ve had kind of an aging physician workforce that has been retiring,” said Todd Patterson, CEO.
The pandemic was difficult for health workers. Many endured long hours, and the stresses on the nation’s health care system prompted more workers than usual to quit or retire.
“There’s a chunk of workers that were lost and won’t come back,” said Joanne Spetz, who directs the Institute for Health Policy Studies at the University of California-San Francisco. “For a lot of the clinicians that decided and were able to stick it out and work through the pandemic, they have burned out,” Spetz said.
Five years after the World Health Organization declared covid a global pandemic and the first Trump administration announced a national emergency, the United States faces a crucial shortage of medical providers, below the projected need for an aging population.
That could have lasting effects on care, particularly in states like Iowa with significant rural populations. Experts say the problem has been building for a while, but the effects of the pandemic accelerated the shortages by pushing many doctors over the edge into early retirement or other fields.
“Some of them made it through covid like ‘Let’s get us through this public health crisis,’ and then they came out of it saying, ‘OK, and now? Now I’m exhausted,’” said Christina Taylor, president of the Iowa Medical Society.
“Iowa is absolutely in the middle of a physician shortage,” Taylor said. “It’s a true crisis for us. We’re actually 44th in the country in terms of patient-to-physician ratio.”
A 2022 survey by the Centers for Disease Control and Prevention found a significant jump in health workers who reported feeling burned out and wanting a new job, compared with 2018. The number of people in health care has grown since the start of the pandemic, said Janette Dill, an associate professor at the University of Minnesota’s School of Public Health, but the growth has not happened fast enough.
“We have an aging population. We have a lot of needs,” she said.
The Association of American Medical Colleges projected last year that the U.S. faces a shortage of up to 86,000 physicians by 2036 — if lawmakers don’t invest more money in training doctors.
These shortages could push more people to seek care in ERs when they can’t see a local doctor, said Michael Dill, director of workforce studies at the AAMC.
“We’re already at a point where tens of millions of Americans every year can’t get medical care when they need it,” said Dill (no relation to Janette Dill). “If the shortage is sustained or gets even worse, then that problem gets worse too, and it disproportionately negatively impacts the most vulnerable amongst us.”
Iowa lawmakers made addressing the shortage a priority in the current legislative session. They introduced bills aimed at increasing medical student loan forgiveness and requesting federal help to add residency training slots for medical students in the state.
Last year, Gov. Kim Reynolds signed a bill into law that drops the residency requirement for some doctors who trained abroad to get a medical license. Lawmakers in at least eight other states have approved similar changes.
Patterson, of the Washington County hospital, appreciates that Iowa lawmakers are trying to increase the pipeline of doctors into Iowa but said it doesn’t address immediate shortages.
“You have a high school student who’s graduating right now; they’re probably nine to 11 years away from entering the workforce as a practicing physician. So it’s a long-term kind of problem,” he said.
For nurses, workforce experts say, the projected national outlook isn’t as dire as in recent years.
“Nursing education is back up. Nursing employment rates are back up. I think, for that workforce, we’ve largely nationally recovered from all the dislocations that occurred,” said Spetz, of the Institute for Health Policy Studies.
But getting nurses to move to the places that need them, like rural communities, will be difficult, she said.
Some rural hospitals in Iowa say an even bigger challenge right now is finding nurses to hire.

Some of that can be traced to the pandemic, said Sara Bruns, nurse manager at Keokuk County Hospital and Clinics. She recalled that some covid patients in critical condition died when they couldn’t be transferred to larger hospitals with more advanced intensive care unit equipment, because those hospitals didn’t have the staff to take on more patients.
“We had to make the horrible decision of ‘You’re probably not going to make it,’” Bruns recalled, saying many patients were then listed as DNR, for “do not resuscitate.”
“That took a big toll on a lot of nurses,” she said.
Another problem is persuading the area’s young nurses to stay, when they would rather live and work in more urban areas, Bruns said.
Her hospital still relies on contracts with travel nurses to fill some night shifts. That’s something the hospital never had to do before the pandemic, Bruns said. Travel nurses are more expensive, adding stress to a small hospital’s budget.
“I think some people just completely got out of nursing,” Bruns said. The pandemic took a special toll “because of the hours that they had to work, the conditions that they had to work.”
Policymakers and health care organizations can’t focus only on recruiting workers, according to Janette Dill at the University of Minnesota. “You also have to retain workers,” she said. “You can’t just recruit new people and then have them be miserable.”
Dill said workers report feeling that patients have been more disrespectful and challenging since the pandemic, and sometimes workers feel unsafe at work. “By ‘unsafe’ I mean physically unsafe. I think that is a very stressful part of the job,” she said.
Research has shown health workers reporting higher levels of burnout and poor mental health since the pandemic — though the risks decreased if workers felt supported by their managers.
Gail Grimes, an intensive care nurse in Des Moines, felt more supported by her employer during the worst parts of the pandemic than she does now, she said. Some hospitals offered pay bumps and more scheduling flexibility to keep nurses on staff.
“We were getting better bonus pay,” Grimes recalled. “We were getting these specialized contracts we could fulfill that were often more worth our time to be able to come in, to miss our families and be there.”
Grimes said she’s seen nurses leave Iowa for neighboring states with better average pay. This creates shortages that she believes affect the care she gives her own patients.
“A nurse taking care of five patients will always be able to provide better care than a nurse taking care of 10 patients,” she said.
She thinks many hospitals have simply accepted staff burnout as a fact, rather than try to prevent it.
“It really is significantly impactful to your mental health when you come home every day and you feel guilty about the things you have not been able to provide to people,” she said.
This article is from a partnership that includes IPR, NPR, and KFF Health News.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).

Watch: Why Insurance Companies Are Denying Coverage for Prosthetic Limbs
PBS News Weekend’s Ali Rogin spoke with KFF Health News contributor Michelle Andrews about what some people with missing limbs consider a disparity in health insurance coverage: Though a knee replacement likely would be covered, a prosthetic knee isn’t always. A prosthetic device can be […]
Health Care
More than 100 new measles cases reported in Ontario as total reaches 925
Measles has spread to 109 more people in Ontario over the last week, bringing the province’s total cases to 925 since an outbreak began in October.
Measles
Beyond Ivy League, RFK Jr.’s NIH Slashed Science Funding Across States That Backed Trump
The National Institutes of Health’s sweeping cuts of grants that fund scientific research are inflicting pain almost universally across the U.S., including in most states that backed President Donald Trump in the 2024 election. A KFF Health News analysis underscores that the terminations are sparing […]
Rural Health
Quebec on verge of declaring measles outbreak over after no new cases in weeks
Quebec’s ministry of health says it’s on the verge of declaring its measles outbreak over, just as cases reach new heights in other parts of the country.
Measles
In Rural Massachusetts, Patients and Physicians Weigh Trade-Offs of Concierge Medicine
Michele Andrews had been seeing her internist in Northampton, Massachusetts, a small city two hours west of Boston, for about 10 years. She was happy with the care, though she started to notice it was becoming harder to get an appointment. “You’d call and you’re […]
Health CareMichele Andrews had been seeing her internist in Northampton, Massachusetts, a small city two hours west of Boston, for about 10 years. She was happy with the care, though she started to notice it was becoming harder to get an appointment.
“You’d call and you’re talking about weeks to a month,” Andrews said.
That’s not surprising, as many workplace surveys show the supply of primary care doctors has fallen well below the demand, especially in rural areas such as western Massachusetts. But Andrews still wasn’t prepared for the letter that arrived last summer from her doctor, Christine Baker, at Pioneer Valley Internal Medicine.
“We are writing to inform you of an exciting change we will be making in our Internal Medicine Practice,” the letter read. “As of September 1st, 2024, we will be switching to Concierge Membership Practice.”
Concierge medicine is a business model in which a doctor charges patients a monthly or annual membership fee — even as the patients continue paying insurance premiums, copays, and deductibles. In exchange for the membership fee, doctors limit their number of patients.
Many physicians who’ve made the change said it resolved some of the pressures they faced in primary care, such as having too many patients to see in too short a time.
Andrews was floored when she got the letter. “The second paragraph tells me the yearly fee for joining will be $1,000 per year for existing patients. It’ll be $1,500 for new patients,” she said.
Although numbers are not tracked in any one place, the trade magazine Concierge Medicine Today estimates there are 7,000 to 22,000 concierge physicians in the U.S. Membership fees range from $1,000 to as high as $50,000 a year.
Critics say concierge medicine helps only patients who have extra money to spend on health care, while shrinking the supply of more traditional primary care practices in a community. It can particularly affect rural communities already experiencing a shortage of primary care options.
Andrews and her husband had three months to either join and pay the fee or leave the practice. They left.
“I’m insulted and I’m offended,” Andrews said. “I would never, never expect to have to pay more out of my pocket to get the kind of care that I should be getting with my insurance premiums.”
Baker, Andrews’ former physician, said fewer than half her patients opted to stay — shrinking her patient load from 1,700 to around 800, which she considers much more manageable. Baker said she had been feeling so stressed that she considered retiring.
“I knew some people would be very unhappy. I knew some would like it,” she said. “And a lot of people who didn’t sign up said, ‘I get why you’re doing it.’”
Patty Healey, another patient at Baker’s practice, said she didn’t consider leaving.
“I knew I had to pay,” Healey said. As a retired nurse, Healey knew about the shortages in primary care, and she was convinced that if she left, she’d have a very difficult time finding a new doctor. Healey was open to the idea that she might like the concierge model.
“It might be to my benefit, because maybe I’ll get earlier appointments and maybe I’ll be able to spend a longer period of time talking about my concerns,” she said.
This is the conundrum of concierge medicine, according to Michael Dill, director of workforce studies at the Association of American Medical Colleges. The quality of care may go up for those who can and do pay the fees, Dill said. “But that means fewer people have access,” he said. “So each time any physician makes that switch, it exacerbates the shortage.”
His association estimates the U.S. will face a shortage of 20,200 to 40,400 primary care doctors within the next decade.
A state analysis found that the percentage of residents in western Massachusetts who said they had a primary care provider was lower than in several other regions of the state.
Dill said the impact of concierge care is worse in rural areas, which often already experience physician shortages. “If even one or two make that switch, you’re going to feel it,” Dill said.
Rebecca Starr, an internist who specializes in geriatric care, recently started a concierge practice in Northampton.
For many years, she consulted for a medical group whose patients got only 15 minutes with a primary care doctor, “and that was hardly enough time to review medications, much less manage chronic conditions,” she said.
When Starr opened her own medical practice, she wanted to offer longer appointments — but still bring in enough revenue to make the business work.
“I did feel a little torn,” Starr said. While it was her dream to offer high-quality care in a small practice, she said, “I have to do it in a way that I have to charge people, in addition to what insurance is paying for.”
Starr said her fee is $3,600 a year, and her patient load will be capped at 200, much lower than the 1,000 or even 2,000 patients that some doctors have. But she still hasn’t hit her limit.
“Certainly there’s some people that would love to join and can’t join because they have limited income,” Starr said.

Many doctors making the switch to concierge medicine say the membership model is the only way to have the kind of personal relationships with patients that attracted them to the profession in the first place.
“It’s a way to practice self-preservation in this field that is punishing patients and doctors alike,” said internal medicine physician Shayne Taylor, who recently opened a practice offering “direct primary care” in Northampton. The direct primary care model is similar to concierge care in that it involves charging a recurring fee to patients, but direct care bypasses insurance companies altogether.
Taylor’s patients, capped at 300, pay her $225 a month for basic primary care visits — and they must have health insurance to cover care such as X-rays and medications, which her practice does not provide. But Taylor doesn’t accept insurance for any of her services, which saves her administrative costs.
“We get a lot of pushback because people are saying, ‘Oh, this is elitist, and this is only going to be accessible to people that have money,’” Taylor said.
But she said the traditional primary care model doesn’t work. “We cannot spend so much time seeing so many patients and documenting in such a way to get an extra $17 from the insurance company.”
While much of the pushback on the membership model comes from patients and policy experts, some of the resistance comes from physicians.
Paul Carlan, a primary care doctor who runs Valley Medical Group in western Massachusetts, said his practice is more stretched than ever. One reason is that the group’s clinics are absorbing some of the patients who have lost their doctor to concierge medicine.
“We all contribute through our tax dollars, which fund these training programs,” Carlan said.
“And so, to some degree, the folks who practice health care in our country are a public good,” Carlan said. “We should be worried when folks are making decisions about how to practice in ways that reduce their capacity to deliver that good back to the public.”
But Taylor, who has the direct primary care practice, said it’s not fair to demand that individual doctors take on the task of fixing a dysfunctional health care system.
“It’s either we do something like this,” Taylor said, “or we quit.”
This article is from a partnership that includes New England Public Media, NPR, and KFF Health News.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).

Alberta health officials warn of possible measles exposure in Calgary, Banff, Canmore
Alberta Health Services has issued a public alert about possible exposure to a confirmed case of measels in the communities of Calgary, Banff and Canmore.
MeaslesLas familias de jóvenes trans ya no ven a Colorado como un refugio para la atención de afirmación de género
GRAND JUNCTION, Colorado — Un viernes después de la escuela, Esa Rodrigues, de 6 años, deshizo un ovillo de lana, asustó a su gato, preguntó a sus familiares sobre sus colores favoritos y delató a su hermano por llamarla “rata chismosa cara de trasero”. Luego, […]
Rural HealthGRAND JUNCTION, Colorado — Un viernes después de la escuela, Esa Rodrigues, de 6 años, deshizo un ovillo de lana, asustó a su gato, preguntó a sus familiares sobre sus colores favoritos y delató a su hermano por llamarla “rata chismosa cara de trasero”.
Luego, se concentró en abrir con los dientes un brillo labial con sabor a cereza.
“¡Sí!”, exclamó, cuando logró abrir la tapa. Esa se puso el brillo en su habitación, donde colgaba en la pared una gran bandera del orgullo transgénero.
Esa dijo que la bandera la hace sentir “importante” y “feliz”. Le gustaría quitarla de la pared y usarla como capa.
Al principio, sus padres cuestionaron su identidad, pero ya no. Antes, su hija, ansiosa, temía ir a la escuela, lloraba en la barbería cuando le hacían un corte “varonil”, y se acurrucó en posición fetal en el suelo del baño cuando supo que nunca tendría la menstruación.
Ahora, esa niña vive la vida con entusiasmo, preguntándose en voz alta si las hadas viven en la casita de cerámica que encontró encaramada en una piedra.
Su madre, Brittni Packard Rodrigues, quiere que esta alegría y aceptación perduren. Dependiendo de la combinación del deseo de Esa, las recomendaciones de sus médicos y el inicio de la pubertad, esto podría requerir bloqueadores, seguidos de estrógeno, para que Esa pueda desarrollar el cuerpo que se adapte a su ser.
“A largo plazo, los bloqueadores ayudan a prevenir todas esas cirugías y procedimientos que podrían convertirse en su realidad si no recibimos esa atención”, dijo Packard Rodrigues.
Los medicamentos conocidos como bloqueadores de la pubertad se usan ampliamente para afecciones como el cáncer de próstata, la endometriosis, la infertilidad y la pubertad precoz. Ahora, la administración Trump busca limitar su uso específicamente para jóvenes transgénero.
Colorado, el estado natal de Esa, es reconocido desde hace tiempo como un refugio para la atención de afirmación de género: se considera legalmente protegida y un beneficio esencial del seguro médico.
En los últimos años, “exiliados médicos” se han mudado a Colorado para recibir este tratamiento. Ya en la década de 1970, el pueblo de Trinidad se hizo conocida como “la capital mundial del cambio de sexo” cuando Stanley Biber, un ex cirujano del ejército con sombrero de vaquero, dejó su huella realizando estas cirugías en adultos.
En su primer día en el cargo, el presidente Donald Trump firmó una orden ejecutiva que refuta la existencia de personas transgénero, argumentando que es una “afirmación falsa que los hombres puedan identificarse como mujeres y, por lo tanto, convertirse en mujeres, y viceversa”.
A la semana siguiente, emitió otra orden que calificaba los bloqueadores de la pubertad y las hormonas para menores de 19 años como una forma de “mutilación” química y “una mancha en la historia de nuestra nación”. La orden instruía a las agencias a tomar medidas para garantizar que los beneficiarios de subvenciones federales para investigación o educación dejaran de proporcionarlos.
Organizaciones de atención médica en Colorado, California, Washington, D.C. y otros lugares anunciaron que cumplirían con la orden preventivamente.
En Colorado, esto incluía a tres importantes organizaciones de atención médica: Children’s Hospital Colorado, Denver Health y UCHealth.
Entre finales de enero y principios de febrero, los tres sistemas anunciaron cambios en la atención de afirmación de género que ofrecían a pacientes menores de 19 años, con efecto inmediato.
Dijeron que ya no recetarían nuevas hormonas ni bloqueadores de la pubertad para pacientes que no los hubieran recibido previamente, se limitarían o no se renovarían las recetas para quienes sí los hubieran recibido, y no se realizarían cirugías. Esto último aunque el Children’s Hospital nunca las había ofrecido, y este tipo de cirugía es poco común en adolescentes: por cada 100.000 menores trans, menos de tres se someten a ella.
![]()
El hospital infantil y Denver Health reanudaron la oferta de bloqueadores de la pubertad y hormonas el 24 y el 19 de febrero, respectivamente, después que Colorado se uniera a una demanda presentada ante el tribunal de distrito de EE. UU. en el estado de Washington.
El tribunal concluyó que las órdenes de Trump relacionadas con el género “discriminan por motivos de condición transgénero y sexo”. Otorgó una orden judicial preliminar que impide su entrada en vigencia en los cuatro estados involucrados.
Sin embargo, las cirugías no se han reanudado. Denver Health afirmó que “mantendrá la pausa en las cirugías de afirmación de género para pacientes menores de 19 años debido a la seguridad del paciente y dada la incertidumbre del panorama legal y regulatorio”.
UCHealth no ha reanudado ni la medicación ni la cirugía para menores de 19 años. “Nuestros proveedores esperan una decisión más definitiva de los tribunales federales que pueda resolver la incertidumbre en torno a la prestación de esta atención”, escribió la vocera Kelli Christensen.
Los jóvenes trans y sus familias afirmaron que el fallo judicial y las decisiones de los dos sistemas de salud de Colorado de reanudar los tratamientos no han resuelto el problema. Les ha dado tiempo para acumular recetas, para intentar encontrar médicos privados con la formación adecuada para supervisar los análisis de sangre, y ajustar las recetas en consecuencia, y, en algunos casos, para resolver la logística de mudarse a otro estado o país.
La administración Trump ha seguido presionando a los proveedores de salud más allá de las órdenes ejecutivas iniciales, amenazando con retener o cancelar los fondos federales que se les habían otorgado. A principios de marzo, la Administración de Recursos y Servicios de Salud (RHSA) anunció que revisaría la financiación de la educación médica de posgrado en hospitales pediátricos.
KFF Health News solicitó comentarios a Kush Desai, subsecretario de prensa de la Casa Blanca, pero no recibió respuesta. La subsecretaria de prensa del Departamento de Salud y Servicios Sociales (HHS), Emily Hilliard, respondió con enlaces a dos comunicados de prensa anteriores.
![]()
Las intervenciones médicas son solo un tipo de atención de afirmación de género, y el proceso para obtener el tratamiento es largo y exhaustivo.
Investigadores han descubierto que, incluso entre quienes tienen seguro médico privado, es poco probable que los jóvenes transgénero reciban bloqueadores de la pubertad ni hormonas. Curiosamente, la mayoría de las cirugías de reducción de senos para afirmación de género realizadas en hombres y menores se practican en pacientes cisgénero, no transgénero.
Kai, de 14 años, quisiera haber podido tomar bloqueadores de la pubertad. Vive en Centennial, un suburbio de Denver. KFF Health News no divulga su nombre completo porque a su familia le preocupa que pueda sufrir acoso.
Kai tuvo su primera menstruación a los 8 años. Para el momento en el que se dio cuenta de que era transgénero, en la secundaria, ya era demasiado tarde para empezar a tomar bloqueadores de la pubertad.
Sus médicos le recetaron anticonceptivos para suprimir sus períodos, así no le recordaban cada mes su disforia de género. Luego, al cumplir los 14, empezó a tomar testosterona.
Kai dijo que si no estuviera en terapia hormonal ahora, sería un peligro para sí mismo.
“Poder decir que estoy feliz con mi cuerpo y poder ser feliz en público sin pensar que todos me miran raro, es una gran diferencia”, dijo.
Su madre, Sherry, dijo que se alegra de ver a Kai relajarse y convertirse en la persona que es.
Sherry, quien pidió usar su segundo nombre para evitar que se identificara a su familia, dijo que comenzó a guardar testosterona en cuanto Trump fue elegido, pero no había pensado en el impacto que esto tendría en la disponibilidad de anticonceptivos. Sin embargo, después de las órdenes ejecutivas, esa receta también se volvió difícil de conseguir. Sherry dijo que el médico de Kai en UCHealth tuvo que programar una reunión especial para confirmar que podía seguir recetándosela.
Así que, por ahora, Kai tiene lo que necesita. Pero para Sherry, eso no es un gran consuelo.
![]()
“No creo que estemos muy seguros”, dijo. “Son solo prórrogas”.
La familia está ideando un plan para salir del país. Si Sherry y su esposo consiguen trabajo en Nueva Zelanda, se mudarán allí. Sherry dijo que esa posibilidad es un privilegio que muchos otros no tienen.
Por ejemplo, David, un estudiante de 18 años de la Universidad Western Colorado en Gunnison, un pueblo de las Montañas Rocallosas, pidió ser identificado solo por su segundo nombre porque le preocupa ser objeto de persecución en este pueblo rural y conservador.
David no tiene pasaporte, pero incluso si lo tuviera, no quiere irse de Gunnison, dijo. Está estudiando geología y aprendiendo a tocar el bajo.
Y tiene un buen grupo de amigos. Planea ser paleontólogo.
Los estantes de su dormitorio están llenos de sus artículos esenciales: fósiles, desodorante Old Spice, macarrones con queso para microondas. Pero no hay espejos. David dijo que se acostumbró a evitarlos.
“Durante mucho tiempo, tuve tanta disforia corporal y dismorfia que puede ser un poco difícil mirarme al espejo”, dijo David. “Pero cuando lo hago, la mayoría de las veces, veo algo que realmente me gusta”.
Lleva tres años tomando testosterona, y la hormona le ayudó a que creciera su barba. En enero, le dijeron a su médico de Denver Health que dejara de recetársela. Su madre condujo horas desde su casa hasta Gunnison para darle la noticia en persona.
La receta ya está activa de nuevo, pero la mastectomía que había planeado para este verano no. Esperaba tener un tiempo de recuperación adecuado antes de empezar el segundo año de la universidad. Pero no conoce a nadie en Colorado que lo haga antes de los 19 años. Podría operarse fácilmente para aumentar sus pechos, pero debe buscar opciones quirúrgicas en otros estados para reducirlos o extirparlos.
“Se suponía que Colorado, como estado, era un refugio”, dijo su madre, Louise, quien pidió ser identificada por su segundo nombre. “Tenemos una ley que otorga a las personas trans el derecho a la atención médica, y sin embargo, nuestros sistemas de salud se la están quitando”.
Han sido necesarios ocho años y unos diez profesionales médicos y terapeutas para que David esté tan cerca de la meta. Es un gran logro después de haber vivido tantos años de disforia y dismorfia.
“Sigo adelante, y seguiré adelante, y casi nada podrá detenerme, porque así soy”, dijo David. “Siempre ha habido personas trans y siempre las habrá”.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).

Deportation Fears Add to Mental Health Problems Confronting Colorado Resort Town Workers
SILVERTHORNE, Colo. — When Adolfo Román García-Ramírez walks home in the evening from his shift at a grocery store in this central Colorado mountain town, sometimes he thinks back on his childhood in Nicaragua. Adults, he recollects, would scare the kids with tales of the […]
Rural Health
States Push Medicaid Work Rules, but Few Programs Help Enrollees Find Jobs
For many years, Eric Wunderlin’s health issues made it hard to find stable employment. Struggling to manage depression and diabetes, Wunderlin worked part-time, minimum-wage retail jobs around Dayton, Ohio, making so little he said he sometimes had to choose between paying rent and buying food. […]
Health CareFor many years, Eric Wunderlin’s health issues made it hard to find stable employment.
Struggling to manage depression and diabetes, Wunderlin worked part-time, minimum-wage retail jobs around Dayton, Ohio, making so little he said he sometimes had to choose between paying rent and buying food.
But in 2018, his CareSource Medicaid health plan offered him help getting a job. It connected him to a life coach, who helped him find full-time work with health benefits. Now, he works for a nonprofit social service agency, a job he said has given him enough financial stability to plan a European vacation next year.
“I feel like a real person and I can go do things,” said Wunderlin, 42. “I feel like I pulled myself out of that slump.”
Republicans in Congress and several states, including Ohio, Iowa, and Montana, are pushing to implement work requirements for nondisabled adults, arguing a mandate would encourage enrollees to find jobs. And for Republicans pushing to require Medicaid enrollees to work, Wunderlin’s story could be held up as evidence that government health coverage can help people find employment and, ultimately, reduce their need for public assistance.
Yet his experience is rare. Medicaid typically does not offer such help, and when states do try to help, such efforts are limited.
And opponents point out that most Medicaid recipients already have jobs and say such a mandate would only kick eligible people off Medicaid, rather than improve their economic prospects. Nearly two-thirds of Medicaid enrollees work, with most of the rest acting as caregivers, going to school, or unable to hold a job due to disability or illness, according to KFF, a health information nonprofit that includes KFF Health News.
Existing efforts to help Medicaid recipients get a job have seen limited success because there’s not a lot of “room to move the needle,” said Ben Sommers, a professor of health care economics at the Harvard T.H. Chan School of Public Health. Most Medicaid enrollees already work — just not in jobs with health benefits, he said.
“The ongoing argument that some folks make is that there are a lot of people freeloading in Medicaid,” he said. “That’s just not supported by the evidence.”

Using Health Programs To Encourage Work
The GOP-controlled Congress could allow or require states to implement a Medicaid work requirement as part of revamping and downsizing Medicaid. The first Trump administration encouraged those work mandates, but many were struck down by federal judges who said they were illegal under federal law.
Policy experts and state officials say more attention should be paid to investments that have helped people find better jobs — from personalized life coaching to, in some cases, health plans’ directly hiring enrollees.
They argue work requirements alone are not enough. “The move to economic mobility requires a ladder, not a stick,” said Farah Khan, a fellow with the Brookings Institution, a nonpartisan think tank.
While Medicaid work requirements have been debated for decades, the issue has become more heated as 40 states and Washington, D.C., have expanded Medicaid eligibility under the Affordable Care Act to the vast majority of low-income adults. More than 20 million adults have gained coverage as a result — but Republicans are now considering eliminating the billions in extra federal funding that helped states extend eligibility beyond groups including many children, pregnant women, and disabled people.
Only Georgia and Arkansas have implemented mandates that some Medicaid enrollees work, volunteer, go to school, or enroll in job training. But a study Sommers co-authored showed no evidence work requirements in Arkansas’ program led to more people working, in part because most of those who could work already were.
In Arkansas, more than 18,000 people lost coverage under the state’s requirement before the policy was suspended by a federal judge in 2019 after less than a year. Those who lost their Medicaid health care reported being unaware or confused about how to report work hours. Since 2023, Arkansas has been giving Medicaid health plans financial incentives to help enrollees train for jobs, but so far few have taken advantage.
Some plans, including Arkansas Blue Cross and Blue Shield’s, offer members $25 to $65 to complete a “career readiness” certificate. In 2024, some Arkansas health plans offered enrollees educational videos about topics including taxes and cryptocurrency.
Health plans don’t have an incentive to help someone find a better-paying job, because that could mean losing a customer if they then make too much to qualify for Medicaid, said Karin VanZant, a vice president at Clearlink Partners, a health care consulting company.
Rather than offering incentives for providing job training, some states, such as California and Ohio, require the insurance companies that run Medicaid to help enrollees find work.
In Montana, where some lawmakers are pushing to implement work requirements, a promising optional program nearly collapsed after state lawmakers required it be outsourced to private contractors.
Within the program’s first three years, the state paired 32,000 Medicaid enrollees with existing federally funded job training programs. Most had higher wages a year after starting training, the state found.
But enrollment has plummeted to just 11 people, according to the latest data provided by the state’s labor department.
Sarah Swanson, who heads the department, said several of the nonprofit contractors that ran the program shuttered. “There was no real part in this for us to deliver direct services to the folks that walked through our door,” she said. The state hopes to revive job training by allowing the department to work alongside contractors to reach more people.
More from Medicaid Watch
-

The House Speaker’s Eyeing Big Cuts to Medicaid. In His Louisiana District, It’s a Lifeline.
Apr 7, 2025
-

‘If They Cut Too Much, People Will Die’: Health Coalition Pushes GOP on Medicaid Funding
Apr 3, 2025
-

Many People With Disabilities Risk Losing Their Medicaid if They Work Too Much
Mar 25, 2025
The Hunt for Results
State officials say they don’t have much data to track the effectiveness of existing job programs offered by Medicaid plans.
Stephanie O’Grady, a spokesperson for the Ohio Department of Medicaid, said the state does not track outcomes because “the health plans are not employment agencies.”
Officials with CareSource, which operates Medicaid plans in multiple states, say it has about 2,300 Medicaid and ACA marketplace enrollees in its JobConnect program — about 1,400 in Ohio, 500 in Georgia, and 400 in Indiana.
The program connects job seekers with a life coach who counsels them on skills such as “showing up on time, dressing the part for interviews, and selling yourself during the interview,” said Jesse Reed, CareSource’s director of life services in Ohio.


Since 2023, about 800 people have found jobs through the program, according to Josh Boynton, a senior vice president at CareSource. The health plan itself has hired 29 Medicaid enrollees into customer service, pharmacy, and other positions — nearly all full-time with benefits, he said.
In 2022, California started offering nontraditional health benefits through Medicaid — including help finding jobs — for enrollees experiencing homelessness or serious mental illness, or who are otherwise at risk of avoidable emergency room care. As of September, it had served nearly 280,000 enrollees, but the state doesn’t have data on how many became employed.
The University of Pittsburgh Medical Center, which is among the largest private employers in Pennsylvania, running both a sprawling hospital system and a Medicaid plan, has hired over 10,000 of its Medicaid enrollees since 2021 through its training and support services. Among other jobs, they took positions as warehouse workers, customer service representatives, and medical assistants.
The vast majority left low-paying jobs for full-time positions with health benefits, said Dan LaVallee, a senior director of UPMC Health Plan’s Center for Social Impact. “Our Pathways to Work program is a model for the nation,” he said.
Josh Archambault, a senior fellow with the conservative Cicero Institute, said Medicaid should focus on improving the financial health of those enrolled.
While the first Trump administration approved Medicaid work requirements in 13 states, the Biden administration or federal judges blocked all except Georgia’s.
“I don’t think states have been given ample chance to experiment and try to figure out what works,” Archambault said.
KFF Health News senior correspondent Angela Hart contributed to this report.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).