

KFF Health News' 'What the Health?': Cutting Medicaid Is Hard — Even for the GOP
The Host Julie Rovner KFF Health News @jrovner @julierovner.bsky.social Read Julie’s stories. Julie Rovner is chief Washington correspondent and host of KFF Health News’ weekly health policy news podcast, “What the Health?” A noted expert on health policy issues, Julie is the author of the […]
Health Care
Ontario reports almost 200 new measles cases as virus spreads across Canada
That brings the province’s tally of probable and confirmed cases to 1,440 since an outbreak began in October.
Measles
Meet the Florida Group Chipping Away at Public Benefits One State at a Time
PHOENIX — As an Arizona bill to block people from using government aid to buy soda headed to the governor’s desk in April, the nation’s top health official joined Arizona lawmakers in the state Capitol to celebrate its passage. Health and Human Services Secretary Robert […]
Health Care



As Republicans Eye Sweeping Medicaid Cuts, Missouri Offers a Preview
CRESTWOOD, Mo. — The prospect of sweeping federal cuts to Medicaid is alarming to some Missourians who remember the last time the public medical insurance program for those with low incomes or disabilities was pressed for cash in the state. In 2005, Missouri adopted some […]
Health CareCRESTWOOD, Mo. — The prospect of sweeping federal cuts to Medicaid is alarming to some Missourians who remember the last time the public medical insurance program for those with low incomes or disabilities was pressed for cash in the state.
In 2005, Missouri adopted some of the strictest eligibility standards in the nation, reduced benefits, and increased patients’ copayments for the joint federal-state program due to state budget shortfalls totaling about $2.4 billion over several prior years. More than 100,000 Missourians lost coverage as a result, and the Federal Reserve Bank of Philadelphia reported that the changes led to increases in credit card borrowing and debt in third-party collections.
A woman told NPR that year that her $6.70-an-hour McDonald’s job put her over the new income limits and rendered her ineligible, even though she was supporting three children on about $300 a week. A woman receiving $865 a month in disability payments worried at a town hall meeting about not being able to raise her orphaned granddaughter as the state asked her to pay $167 a month to keep her health coverage.
Now, Missouri could lose an estimated $2 billion a year in federal funding as congressional Republicans look to cut at least $880 billion over a decade from a pool of funding that includes Medicaid programs nationwide. Medicaid and the closely related Children’s Health Insurance Program together insure roughly 79 million people — about 1 in 5 Americans.
“We’re looking at a much more significant impact with the loss of federal funds even than what 2005 was,” said Amy Blouin, president of the progressive Missouri Budget Project think tank. “We’re not going to be able to protect kids. We’re not going to be able to protect people with disabilities from some sort of impact.”
At today’s spending levels, a cut of $880 billion to Medicaid could lead to states’ losing federal funding ranging from $78 million a year in Wyoming to $13 billion a year in California, according to an analysis from KFF, a health information nonprofit that includes KFF Health News. State lawmakers nationwide would then be left to address the shortfalls, likely through some combination of slashing benefits or eligibility, raising taxes, or finding a different large budget item to cut, such as education spending.
Republican lawmakers are floating various proposals to cut Medicaid, including one to reduce the money the federal government sends to states to help cover adults who gained access to the program under the Affordable Care Act’s provision known as Medicaid expansion. The 2010 health care law allowed states to expand Medicaid eligibility to cover more adults with low incomes. The federal government is picking up 90% of the tab for that group. About 20 million people nationwide are now covered through that expansion.
Missouri expanded Medicaid in 2021. That has meant that a single working-age adult in Missouri can now earn up to $21,597 a year and qualify for coverage, whereas before, nondisabled adults without children couldn’t get Medicaid coverage. That portion of the program now covers over 329,000 Missourians, more than a quarter of the state’s Medicaid recipients.
For every percentage point that the federal portion of the funding for that group decreases, Missouri’s Medicaid director estimated, the state could lose $30 million to $35 million a year.
But the equation is even more complicated given that Missouri expanded access via a constitutional amendment. Voters approved the expansion in 2020 after the state’s Republican leadership resisted doing so for a decade. That means changes to Medicaid expansion in Missouri would require voters to amend the state constitution again. The same is true in South Dakota and Oklahoma.
So even if Congress attempted to narrowly target cuts to the nation’s Medicaid expansion population, Washington University in St. Louis health economist Timothy McBride said, Missouri’s expansion program would likely stay in place.
“Then you would just have to find the money elsewhere, which would be brutal in Missouri,” McBride said.
In Crestwood, a suburb of St. Louis, Sandra Smith worries her daughter’s in-home nursing care would be on the chopping block. Nearly all in-home services are an optional part of Medicaid that states are not required to include in their programs. But the services have been critical for Sandra and her 24-year-old daughter, Sarah.
Sarah Smith has been disabled for most of her life due to seizures from a rare genetic disorder called Dravet syndrome. She has been covered by Medicaid in various ways since she was 3.

She needs intensive, 24-hour care, and Medicaid pays for a nurse to come to their home 13 hours a day. Her mother serves as the overnight caregiver and covers when the nurses are sick — work Sandra Smith is not allowed to be compensated for and that doesn’t count toward the 63-year-old’s Social Security.
Having nursing help allows Sandra Smith to work as an independent podcast producer and gives her a break from being the go-to-person for providing care 24 hours a day, day after day, year after year.
“I really and truly don’t know what I would do if we lost the Medicaid home care. I have no plan whatsoever,” Sandra Smith said. “It is not sustainable for anyone to do infinite, 24-hour care without dire physical health, mental health, and financial consequences, especially as we parents get into our elder years.”
Elias Tsapelas, director of fiscal policy at the conservative Show-Me Institute, said potential changes to Medicaid programs depend on the extent of any budget cuts that Congress ultimately passes and how much time states have to respond.
A large cut implemented immediately, for example, would require state legislators to look for parts of the budget they have the discretion to cut quickly. But if states have time to absorb funding changes, he said, they would have more flexibility.
“I’m not ready to think that Congress is going to willingly put us on the path of making every state go cut their benefits for the most vulnerable,” Tsapelas said.
Missouri’s congressional delegation split along party lines over the recent budget resolution calling for deep spending cuts, with the Republicans who control six of the eight House seats and both Senate seats all voting for it.
But 76% of the public, including 55% of Republicans, say they oppose major federal funding cuts to Medicaid, according to a national KFF poll conducted April 8-15.
And Missouri Sen. Josh Hawley, a Republican, has said that he does not support cutting Medicaid and posted on the social platform X that he was told by President Donald Trump that the House and Senate would not cut Medicaid benefits and that Trump won’t sign any benefit cuts.
“I hope congressional leadership will get the message,” Hawley posted. He declined to comment for this article.
U.S. House Republicans are aiming to pass a budget by Memorial Day, after many state legislatures, including Missouri’s, will have adjourned for the year.
Meanwhile, Missouri lawmakers are poised to pass a tax cut that is estimated to reduce state revenue by about $240 million in the first year.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).

Nova Scotia resident becomes province’s 1st measles case in 2 years after U.S. visit
Public health has released a list of possible exposure locations in downtown Halifax, including a hotel, a bar and the Halifax Infirmary ER.
Measles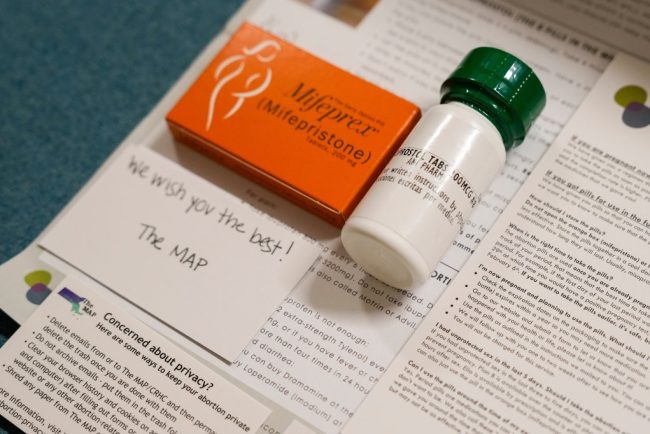
Despite Historic Indictment, Doctors Will Keep Mailing Abortion Pills Across State Lines
When the news broke on Jan. 31 that a New York physician had been indicted for shipping abortion medications to a woman in Louisiana, it stoked fear across the network of doctors and medical clinics who engage in similar work. “It’s scary. It’s frustrating,” said […]
Pharmaceuticals
At Social Security, These Are the Days of the Living Dead
Rennie Glasgow, who has served 15 years at the Social Security Administration, is seeing something new on the job: dead people. They’re not really dead, of course. In four instances over the past few weeks, he told KFF Health News, his Schenectady, New York, office […]
Health Care
HIV Testing and Outreach Falter as Trump Funding Cuts Sweep the South
JACKSON, Miss. — Storm clouds hung low above a community center in Jackson, where pastor Andre Devine invited people inside for lunch. Hoagies with smoked turkey and ham drew the crowd, but several people lingered for free preventive health care: tests for HIV and other […]
Health CareJACKSON, Miss. — Storm clouds hung low above a community center in Jackson, where pastor Andre Devine invited people inside for lunch. Hoagies with smoked turkey and ham drew the crowd, but several people lingered for free preventive health care: tests for HIV and other diseases, flu shots, and blood pressure and glucose monitoring.
Between greetings, Devine, executive director of the nonprofit group Hearts for the Homeless, commiserated with his colleagues about the hundreds of thousands of dollars their groups had lost within a couple of weeks, swept up in the Trump administration’s termination of research dollars and clawback of more than $11 billion from health departments across the country.
Devine would have to scale back food distribution for people in need. And his colleagues at the nonprofit health care group My Brother’s Keeper were worried they’d have to shutter the group’s mobile clinic — an RV offering HIV tests, parked beside the community center that morning. Several employees had already been furloughed and the cuts kept coming, said June Gipson, CEO of My Brother’s Keeper.
“People can’t work without being paid,” she said.
The directors of other community-based groups in Mississippi, Alabama, Louisiana, and Tennessee told KFF Health News they too had reduced their spending on HIV testing and outreach because of delayed or slashed federal funds — or they were making plans to do so, anticipating cuts to come.
Scaling back these efforts could prove tragic, Gipson said. Without an extra boost of support to get tested or stay on treatment, many people living with HIV will grow sicker and stand a greater chance of infecting others.
President Donald Trump, in his first term, promised to end America’s HIV epidemic — and he put the resources of the federal government behind the effort. This time, he has deployed the powers of his office to gut funding, abandoning those communities at highest risk of HIV.
Trump’s earlier efforts targeted seven Southern states, including Mississippi, where funds went to community groups and health departments that tailor interventions to historically underserved communities that face discrimination and have less access to quality education, health care, stable income, and generational wealth. Such factors help explain why Black people accounted for 38% of HIV diagnoses in the United States in 2023, despite representing only 14% of the population, and also why half of the country’s new HIV infections occur in the South.
Now, Trump is undermining HIV efforts by barring funds from programs built around diversity, equity, and inclusion. A Day One executive order said they represent “immense public waste and shameful discrimination.”
Since then, his administration has cut millions of dollars in federal grants to health departments, universities, and nonprofit organizations that do HIV work. And in April, it eliminated half of the Centers for Disease Control and Prevention’s 10 HIV branch offices, according to an email to grant recipients, reviewed by KFF Health News, from the director of the CDC’s Division of HIV Prevention. The layoffs included staff who had overseen the rollout of HIV grants to health departments and community-based groups, like My Brother’s Keeper.
The CDC provides more than 90% of all federal funding for HIV prevention — about $1 billion annually. The Trump administration’s May 2 budget proposal for fiscal 2026 takes aim at DEI initiatives, including in its explanation for cutting $3.59 billion from the CDC. Although the proposal doesn’t mention HIV prevention specifically, the administration’s drafted plan for HHS, released mid-April, eliminates all prevention funding at the CDC, as well as funding for Trump’s initiative to end the epidemic.
Eliminating federal funds for HIV prevention would lead to more than 143,000 additional people in the U.S. becoming infected with HIV within five years, and about 127,000 additional people who die of AIDS-related causes, according to estimates from the Foundation for AIDS Research, a nonprofit known as amfAR. Excess medical costs would exceed $60 billion, it said.
Eldridge Dwayne Ellis, the coordinator of the mobile testing clinic at My Brother’s Keeper, said curbing the group’s services goes beyond HIV.
“People see us as their only outlet, not just for testing but for confidential conversations, for a shoulder to cry on,” he said. “I don’t understand how someone, with the stroke of a pen, could just haphazardly write off the health of millions.”
Quiet Tears
Ellis came into his role in the mobile clinic haphazardly, when he worked as a construction worker. Suddenly dizzy and unwell on a job, a co-worker suggested he visit the organization’s brick-and-mortar clinic nearby. He later applied for a position with My Brother’s Keeper, inspired by its efforts to give people support to help themselves.
For example, Ellis described a young man who visited the mobile clinic recently who had been kicked out of his home and was sleeping on couches or on the street. Ellis thought of friends he’d known in similar situations that put them at risk of HIV by increasing the likelihood of transactional sex or substance use disorders.
When a rapid test revealed HIV, the young man fell silent. “The quiet tears hurt worse — it’s the dread of mortality,” Ellis said. “I tried to be as strong as possible to let him know his life is not over, that this wasn’t a death sentence.”
Ellis and his team enrolled the man into HIV care that day and stayed in touch. Otherwise, Ellis said, he might not have had the means or fortitude to seek treatment on his own and adhere to daily HIV pills. Not only is that deadly for people with HIV, it’s bad for public health. HIV experts use the phrase “treatment as prevention” because most new infections derive from people who aren’t adhering to treatment well enough to be considered virally suppressed — which keeps the disease from spreading.
Only a third of people living with HIV in Mississippi were virally suppressed in 2022. Nationally, that number is about 65%. That’s worse than in eastern and southern Africa, where 78% of people with HIV aren’t spreading the virus because they’re on steady treatment.
My Brother’s Keeper is one of many groups improving such numbers by helping people get tested and stay on medication. But the funding cuts in Washington have curtailed their work. The first loss was a $12 million grant from the National Institutes of Health, not even two years into a 10-year project. “Programs based primarily on artificial and non-scientific categories, including amorphous equity objectives, are antithetical to the scientific inquiry,” the NIH said in a letter reviewed by KFF Health News.
My Brother’s Keeper then lost a CDC award to reduce health disparities — a grant channeled through the Mississippi state health department — that began with the group’s work during the covid pandemic but had broadened to screening and care for HIV, heart disease, and diabetes. These are some of the maladies that account for why low-income Black people in the Deep South die sooner, on average, than those who are white. According to a recent study, the former’s life expectancy was just 68 years in 2021, on par with the average in impoverished nations like Rwanda and Myanmar.
The group then lost CDC funding that covered the cost of laboratory work to detect HIV, chlamydia, gonorrhea, and syphilis in patients’ blood samples. Mississippi has the highest rate of sexually transmitted diseases among states, in part because people spread infections when they aren’t tested and treated.
“The labs are $200 to $600 per person,” Gipson said, “so now we can’t do that without passing the cost to the patient, and some can’t pay.”
Two other CDC grants on HIV prevention, together worth $841,000, were unusually delayed.
Public health specialists close to the CDC, who spoke on condition of anonymity because they fear retaliation, said they were aware of delays in HIV prevention funding, despite court orders to unfreeze payments for federal grants in January and February. “The faucet was being turned off at a higher level than at the CDC,” one specialist said. The delays have now been compounded, they said, by the gutting of that agency’s HIV workforce in April.
“I know of many organizations reliant on subcontracted federal funds who have not been paid for the work they’ve done, or whose funding has been terminated,” said Dafina Ward, executive director of the Southern AIDS Coalition.

To reach the underserved, these groups offer food, housing assistance, bus passes, disease screening, and a sense of community. A network of the groups was fostered, in part, by Trump’s initiative to end the epidemic. And it showed promise: From 2017 to 2022, new HIV infections decreased by 21% in the cities and the Southern states it targeted.
Disparities in infections were still massive, with the rate of HIV diagnoses about eight times as high for Black people as white people, and the South remained hardest hit. Ward was hopeful at the start of this year, however, as testing became more widespread and HIV prevention drugs — called preexposure prophylaxis, or PrEP — slowly gained popularity. But her outlook has shifted and she fears that grassroots organizations might not weather the funding turmoil.
“We’re seeing an about-face of what it means to truly work towards ending HIV in this country,” she said.
A Closed Clinic
Southeast of Jackson, in Hattiesburg, Sean Fortenberry tears up as he walks into a small room used until recently for HIV testing. He has kept his job at Mississippi’s AIDS Services Coalition by shifting his role but agonizes about the outcome. When Fortenberry tested positive for HIV in 2007, he said, his family and doctor saved his life.
“I never felt that I was alone, and that was really, really important,” he said. “Other people don’t have that, so when I came across this position, I was gung-ho. I wanted to help.”
But the coalition froze its HIV testing clinic and paused mobile testing at homeless shelters, colleges, and churches late last year. Kathy Garner, the group’s executive director, said the Mississippi health department — which funds the coalition with CDC’s HIV prevention dollars — told her to pause outreach in October before the state renewed the group’s annual HIV prevention contract.
Kendra Johnson, communicable diseases director at Mississippi’s health department, said that delays in HIV prevention funds were initially on the department’s end because it was short on administrative staff. Then Trump took office. “We were working with our federal partners to ensure that our new objectives were in line with new HIV prevention activities,” Johnson said. “And we ran into additional delays due to paused communications at the federal level.”
The AIDS coalition remains afloat largely because of federal money from the Ryan White HIV/AIDS Program for treatment and from the Department of Housing and Urban Development. “If most of these federal dollars are cut, we would have to close,” Garner said.
The group provides housing or housing assistance to roughly 400 people each year. Research shows that people in stable housing adhere much better to HIV treatment and are far less likely to die than unhoused people with HIV.

Funding cuts have shaken every state, but the South is acutely vulnerable when it comes to HIV, said Gregorio Millett, director of public policy at amfAR. Southern states have the highest level of poverty and a severe shortage of rural clinics, and several haven’t expanded Medicaid so that more low-income adults have health insurance.
Further, Southern states aren’t poised to make up the difference. Alabama, Louisiana, Kentucky, Mississippi, and Missouri put zero state funds into HIV prevention last year, according to NASTAD, an association of public health officials who administer HIV and hepatitis programs. In contrast, about 40% of Michigan’s HIV prevention budget is provided by the state, 50% of Colorado’s HIV prevention budget, and 88% of New York’s.
“When you are in the South, you need the federal government,” said Gipson, from My Brother’s Keeper. “When we had slavery, we needed the federal government. When we had the push for civil rights, we needed the federal government. And we still need the federal government for health care,” she said. “The red states are going to suffer, and we’re going to start suffering sooner than anyone else.”
‘So Goes Mississippi’
When asked about cuts and delays to HIV prevention funding, the CDC directed queries to HHS. The department’s director of communications, Andrew Nixon, replied in an email: “Critical HIV/AIDS programs will continue under the Administration for a Healthy America (AHA) as a part of Secretary [Robert F.] Kennedy’s vision to streamline HHS to better serve the American people.”
Nixon did not reply to a follow-up question on whether the Trump administration considers HIV prevention critical.
On April 4, Gipson received a fraction of her delayed HIV prevention funds from the CDC. But Gipson said she was afraid to hire back staff amid the turmoil.
Like the directors of many other community organizations, Gipson is going after grants from foundations and companies. Pharmaceutical firms such as Gilead and GSK that produce HIV drugs are among the largest contributors of non-governmental funds for HIV testing, prevention, and care, but private funding for HIV has never come close to the roughly $40 billion that the federal government allocated to HIV annually.
“If the federal government withdraws some or all of its support, the whole thing will collapse,” said Alice Riener, CEO of the community-based organization CrescentCare in Louisiana. “What you see in Mississippi is the beginning of that, and what’s so concerning is the infrastructure we’ve built will collapse quickly but take decades to rebuild.”

Southern health officials are reeling from cuts because state budgets are already tight. Mississippi’s state health officer, Daniel Edney, spoke with KFF Health News on the day the Trump administration terminated $11 billion in covid-era funds intended to help states improve their public health operations. “There’s not a lot of fat, and we’re cutting it to the bone right now,” Edney said.
Mississippi needed this boost, Edney said, because the state ranks among the lowest in health metrics including premature death, access to clinical care, and teen births. But Edney noted hopeful trends: The state had recently moved from 50th to 49th worst in health rankings, and its rate of new HIV cases was dropping.
“The science tells us what we need to do to identify and care for patients, and we’re improving,” he said. “But trends can change very quickly on us, so we can’t take our foot off the gas pedal.”
If that happens, researchers say, the comeback of HIV will go unnoticed at first, as people at the margins of society are infected silently before they’re hospitalized. As untreated infections spread, the rise will eventually grow large enough to make a dent in national statistics, a resurgence that will cost lives and take years, if not decades, to reverse.
Outside the community center on that stormy March morning, pastor Devine lamented not just the loss of his grant from the health department, but a $1 billion cut to food distribution programs at the U.S. Department of Agriculture. He rattled off consequences he feared: People relying on food assistance would be forced to decide between buying groceries, paying bills, or seeing a doctor, driving them further into poverty, into emergency rooms, into crime.
Deja Abdul-Haqq, a program director at My Brother’s Keeper, nodded along as he spoke. “So goes Mississippi, so goes the rest of the United States,” Abdul-Haqq said. “Struggles may start here, but they spread.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).

Trump Team’s $500 Million Bet on Old Vaccine Technology Puzzles Scientists
The Trump administration’s unprecedented $500 million grant for a broadly protective flu shot has confounded vaccine and pandemic preparedness experts, who said the project was in early stages, relied on old technology, and was just one of more than 200 such efforts. Health and Human […]
Pharmaceuticals
An Arm and a Leg: Why ‘The Pitt’ Is Our Fave New Drama
People who work in real-life emergency rooms have raved about how the new TV drama “The Pitt” accurately captures the complex dynamics of their workplaces and the medical details of their cases. Host Dan Weissmann talks with Alex Janke, an emergency medicine doctor and health […]
Health Care
Measles exposure alert issued for communities south of Winnipeg
Public health officials in Manitoba are warning of new measles exposure sites in two communities south of Winnipeg, including a medical centre and an elementary school.
Measles
Alberta reports 17 more cases of measles, bringing total to more than 200
Measles symptoms include fever, coughing, a runny nose, red eyes and a blotchy, red rash that appears three to seven days after the fever starts.
Measles
Toronto Public Health warns of possible measles exposure at major tourist attraction
Toronto Public Health said that on Monday, April 21, someone with a case of measles had visited Ripley’s Aquarium, beside the CN Tower.
Measles