

An Arm and a Leg: Winning a Two-Year Fight Over a Bogus Bill
In July 2022, “An Arm and a Leg” listener Meagan experienced a bout of vertigo that landed her in the emergency room. For more than two years after, Meagan endured what felt like a never-ending series of communications with the hospital over a medical bill […]
Health Care
Medi-Cal Under Threat: Who’s Covered and What Could Be Cut?
SACRAMENTO, Calif. — Medi-Cal, California’s complex, $174.6 billion Medicaid program, provides health insurance for nearly 15 million residents with low incomes and disabilities. The state enrolls twice as many people as New York and more than three times as many as Texas — the two […]
Health Care
Quebec declares end to measles outbreak after no cases reported for 32 days
Health officials say an outbreak can be considered over if 32 days pass without a new reported infection.
Measles



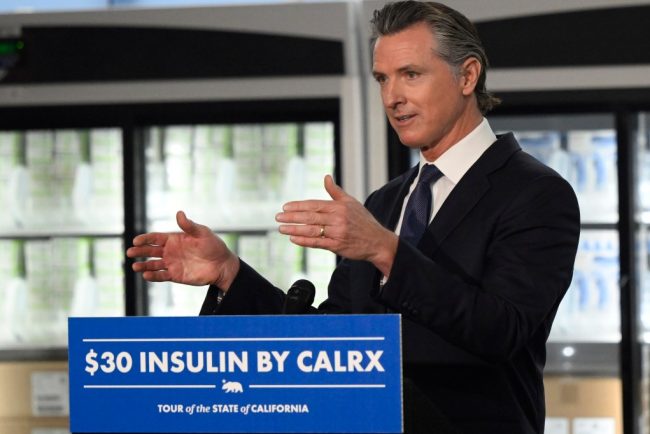
Top California Democrats Clash Over How To Rein In Drug Industry Middlemen
California Gov. Gavin Newsom and state legislators in Sacramento seem to agree: Prescription drug prices are too high. But lawmakers and the second-term governor are at odds over what to do about it, and a recent proposal could trigger one of the biggest health care […]
Pharmaceuticals
Long-Covid Patients Are Frustrated That Federal Research Hasn’t Found New Treatments
Erica Hayes, 40, has not felt healthy since November 2020 when she first fell ill with covid. Hayes is too sick to work, so she has spent much of the last four years sitting on her beige couch, often curled up under an electric blanket. […]
PharmaceuticalsErica Hayes, 40, has not felt healthy since November 2020 when she first fell ill with covid.
Hayes is too sick to work, so she has spent much of the last four years sitting on her beige couch, often curled up under an electric blanket.
“My blood flow now sucks, so my hands and my feet are freezing. Even if I’m sweating, my toes are cold,” said Hayes, who lives in Western Pennsylvania. She misses feeling well enough to play with her 9-year-old son or attend her 17-year-old son’s baseball games.
Along with claiming the lives of 1.2 million Americans, the covid-19 pandemic has been described as a mass disabling event. Hayes is one of millions of Americans who suffer from long covid. Depending on the patient, the condition can rob someone of energy, scramble the autonomic nervous system, or fog their memory, among many other symptoms.In addition to the brain fog and chronic fatigue, Hayes’ constellation of symptoms includes frequent hives and migraines. Also, her tongue is constantly swollen and dry.
“I’ve had multiple doctors look at it and tell me they don’t know what’s going on,” Hayes said about her tongue.
Estimates of prevalence range considerably, depending on how researchers define long covid in a given study, but the Centers for Disease Control and Prevention puts it at 17 million adults.
Despite long covid’s vast reach, the federal government’s investment in researching the disease — to the tune of $1.15 billion as of December — has so far failed to bring any new treatments to market.
This disappoints and angers the patient community, who say the National Institutes of Health should focus on ways to stop their suffering instead of simply trying to understand why they’re suffering.
“It’s unconscionable that more than four years since this began, we still don’t have one FDA-approved drug,” said Meighan Stone, executive director of the Long COVID Campaign, a patient-led advocacy organization. Stone was among several people with long covid who spoke at a workshop hosted by the NIH in September where patients, clinicians, and researchers discussed their priorities and frustrations around the agency’s approach to long-covid research.
Some doctors and researchers are also critical of the agency’s research initiative, called RECOVER, or Researching COVID to Enhance Recovery. Without clinical trials, physicians specializing in treating long covid must rely on hunches to guide their clinical decisions, said Ziyad Al-Aly, chief of research and development with the VA St Louis Healthcare System.
“What [RECOVER] lacks, really, is clarity of vision and clarity of purpose,” said Al-Aly, saying he agrees that the NIH has had enough time and money to produce more meaningful progress.
Now the NIH is starting to determine how to allocate an additional $662 million of funding for long-covid research, $300 million of which is earmarked for clinical trials. These funds will be allocated over the next four years.At the end of October, RECOVER issued a request for clinical trial ideas that look at potential therapies, including medications, saying its goal is “to work rapidly, collaboratively, and transparently to advance treatments for Long COVID.”
This turn suggests the NIH has begun to respond to patients. This has stirred cautious optimism among those who say that the agency’s approach to long covid has lacked urgency in the search for effective treatments.Stone calls this $300 million a down payment. She warns it’s going to take a lot more money to help people like Hayes regain some degree of health.“There really is a burden to make up this lost time now,” Stone said.
The NIH told KFF Health News and NPR via email that it recognizes the urgency in finding treatments. But to do that, there needs to be an understanding of the biological mechanisms that are making people sick, which is difficult to do with post-infectious conditions.
That’s why it has funded research into how long covid affects lung function, or trying to understand why only some people are afflicted with the condition.
Good Science Takes Time
In December 2020, Congress appropriated $1.15 billion for the NIH to launch RECOVER, raising hopes in the long-covid patient community.
Then-NIH Director Francis Collins explained that RECOVER’s goal was to better understand long covid as a disease and that clinical trials of potential treatments would come later.
According to RECOVER’s website, it has funded eight clinical trials to test the safety and effectiveness of an experimental treatment or intervention. Just one of those trials has published results.
On the other hand, RECOVER has supported more than 200 observational studies, such as research on how long covid affects pulmonary function and on which symptoms are most common. And the initiative has funded more than 40 pathobiology studies, which focus on the basic cellular and molecular mechanisms of long covid.
RECOVER’s website says this research has led to crucial insights on the risk factors for developing long covid and on understanding how the disease interacts with preexisting conditions.
It notes that observational studies are important in helping scientists to design and launch evidence-based clinical trials.
Good science takes time, said Leora Horwitz, the co-principal investigator for the RECOVER-Adult Observational Cohort at New York University. And long covid is an “exceedingly complicated” illness that appears to affect nearly every organ system, she said.
This makes it more difficult to study than many other diseases. Because long covid harms the body in so many ways, with widely variable symptoms, it’s harder to identify precise targets for treatment.
“I also will remind you that we’re only three, four years into this pandemic for most people,” Horwitz said. “We’ve been spending much more money than this, yearly, for 30, 40 years on other conditions.”
NYU received nearly $470 million of RECOVER funds in 2021, which the institution is using to spearhead the collection of data and biospecimens from up to 40,000 patients. Horwitz said nearly 30,000 are enrolled so far.
This vast repository, Horwitz said, supports ongoing observational research, allowing scientists to understand what is happening biologically to people who don’t recover after an initial infection — and that will help determine which clinical trials for treatments are worth undertaking.
“Simply trying treatments because they are available without any evidence about whether or why they may be effective reduces the likelihood of successful trials and may put patients at risk of harm,” she said.
Delayed Hopes or Incremental Progress?
The NIH told KFF Health News and NPR that patients and caregivers have been central to RECOVER from the beginning, “playing critical roles in designing studies and clinical trials, responding to surveys, serving on governance and publication groups, and guiding the initiative.”But the consensus from patient advocacy groups is that RECOVER should have done more to prioritize clinical trials from the outset. Patients also say RECOVER leadership ignored their priorities and experiences when determining which studies to fund.
RECOVER has scored some gains, said JD Davids, co-director of Long COVID Justice. This includes findings on differences in long covid between adults and kids.But Davids said the NIH shouldn’t have named the initiative “RECOVER,” since it wasn’t designed as a streamlined effort to develop treatments.
“The name’s a little cruel and misleading,” he said.
RECOVER’s initial allocation of $1.15 billion probably wasn’t enough to develop a new medication to treat long covid, said Ezekiel J. Emanuel, co-director of the University of Pennsylvania’s Healthcare Transformation Institute.
But, he said, the results of preliminary clinical trials could have spurred pharmaceutical companies to fund more studies on drug development and test how existing drugs influence a patient’s immune response.
Emanuel is one of the authors of a March 2022 covid roadmap report. He notes that RECOVER’s lack of focus on new treatments was a problem. “Only 15% of the budget is for clinical studies. That is a failure in itself — a failure of having the right priorities,” he told KFF Health News and NPR via email.
And though the NYU biobank has been impactful, Emanuel said there needs to be more focus on how existing drugs influence immune response.
He said some clinical trials that RECOVER has funded are “ridiculous,” because they’ve focused on symptom amelioration, for example to study the benefits of over-the-counter medication to improve sleep. Other studies looked at non-pharmacological interventions, such as exercise and “brain training” to help with cognitive fog.
People with long covid say this type of clinical research contributes to what many describe as the “gaslighting” they experience from doctors, who sometimes blame a patient’s symptoms on anxiety or depression, rather than acknowledging long covid as a real illness with a physiological basis.
“I’m just disgusted,” said long-covid patient Hayes. “You wouldn’t tell somebody with diabetes to breathe through it.”
Chimére L. Sweeney, director and founder of the Black Long Covid Experience, said she’s even taken breaks from seeking treatment after getting fed up with being told that her symptoms were due to her diet or mental health.
“You’re at the whim of somebody who may not even understand the spectrum of long covid,” Sweeney said.

Insurance Battles Over Experimental Treatments
Since there are still no long-covid treatments approved by the Food and Drug Administration, anything a physician prescribes is classified as either experimental — for unproven treatments — or an off-label use of a drug approved for other conditions. This means patients can struggle to get insurance to cover prescriptions.
Michael Brode, medical director for UT Health Austin’s Post-COVID-19 Program — said he writes many appeal letters. And some people pay for their own treatment.
For example, intravenous immunoglobulin therapy, low-dose naltrexone, and hyperbaric oxygen therapy are all promising treatments, he said.
For hyperbaric oxygen, two small, randomized controlled studies show improvements for the chronic fatigue and brain fog that often plague long-covid patients. The theory is that higher oxygen concentration and increased air pressure can help heal tissues that were damaged during a covid infection.
However, the out-of-pocket cost for a series of sessions in a hyperbaric chamber can run as much as $8,000, Brode said.
“Am I going to look a patient in the eye and say, ‘You need to spend that money for an unproven treatment’?” he said. “I don’t want to hype up a treatment that is still experimental. But I also don’t want to hide it.”
There’s a host of pharmaceuticals that have promising off-label uses for long covid, said microbiologist Amy Proal, president and chief scientific officer at the Massachusetts-based PolyBio Research Foundation. For instance, she’s collaborating on a clinical study that repurposes two HIV drugs to treat long covid.
Proal said research on treatments can move forward based on what’s already understood about the disease. For instance, she said that scientists have evidence — partly due to RECOVER research — that some patients continue to harbor small amounts of viral material after a covid infection. She has not received RECOVER funds but is researching antivirals.
But to vet a range of possible treatments for the millions suffering now — and to develop new drugs specifically targeting long covid — clinical trials are needed. And that requires money.
Hayes said she would definitely volunteer for an experimental drug trial. For now, though, “in order to not be absolutely miserable,” she said she focuses on what she can do, like having dinner with her family.At the same time, Hayes doesn’t want to spend the rest of her life on a beige couch.
RECOVER’s deadline to submit research proposals for potential long-covid treatments is Feb. 1.
This article is from a partnership that includes NPR and KFF Health News.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
Health Care Is Newsom’s Biggest Unfinished Project. Trump Complicates That Task.
SACRAMENTO, Calif. — Six years after he entered office vowing to be California’s “health care governor,” Democrat Gavin Newsom has steered tens of billions in public funding to safety net services for the state’s neediest residents while engineering rules to make health care more accessible […]
Pharmaceuticals La salud, un proyecto inconcluso del gobernador de California
SACRAMENTO, California.— Seis años después de asumir el cargo prometiendo ser el “gobernador de la salud” de California, el demócrata Gavin Newsom ha destinado decenas de miles de millones de dólares de fondos públicos a servicios de la red de seguridad para los residentes más […]
Pharmaceuticals
‘Bill of the Month’: The Series That Dissects and Slashes Medical Bills
Over 6½ years ago, KFF Health News and NPR kicked off “Bill of the Month,” a crowdsourced investigation highlighting the impact of medical bills on patients. The goal was to understand how the U.S. health care system generates outsize bills and to empower patients with […]
PharmaceuticalsOver 6½ years ago, KFF Health News and NPR kicked off “Bill of the Month,” a crowdsourced investigation highlighting the impact of medical bills on patients.
The goal was to understand how the U.S. health care system generates outsize bills and to empower patients with strategies to avoid them. We asked readers and listeners to submit their bills — and they kept coming. “Bill of the Month” has received nearly 10,000 submissions, each a picture of a health system’s dysfunction and the financial burden it places on the patients.
Since 2018, we have analyzed bills totaling almost $6.3 million — including nearly $2.8 million that patients were expected to pay out-of-pocket.
Cited at statehouses and the U.S. Capitol, the series has led to changes in health policy. Two patients featured by “Bill of the Month” were invited to the White House in 2019 to discuss their surprise bills: Elizabeth Moreno’s $18,000 urine test and Drew Calver’s $109,000 heart attack. In 2020, Congress passed the federal No Surprises Act, shielding patients from most out-of-network bills in emergencies, among other protections.

Last year, the Biden administration announced plans to lower health costs that included targeting a loophole that allowed health providers to evade the surprise-billing law — a problem first identified by “Bill of the Month.”
Many patients submitted high prescription drug bills. In treatment for prostate cancer, Paul Hinds was billed nearly $74,000 for two shots of an old drug called Lupron, which can cost just a couple of hundred dollars overseas.
Now, the federal government has identified Lupron as one of the medicines that has seen its price rise faster than inflation — meaning its manufacturer owes rebates to Medicare under President Joe Biden’s 2022 Inflation Reduction Act.
The law also authorized the Biden administration to begin negotiating the price of specified drugs for Medicare patients, who now benefit from a cap on the price of insulin.
“Bill of the Month” has helped many patients and readers get their medical bills reduced or forgiven. Roughly 1 in 3 bills were resolved for patients by the time their features were published.
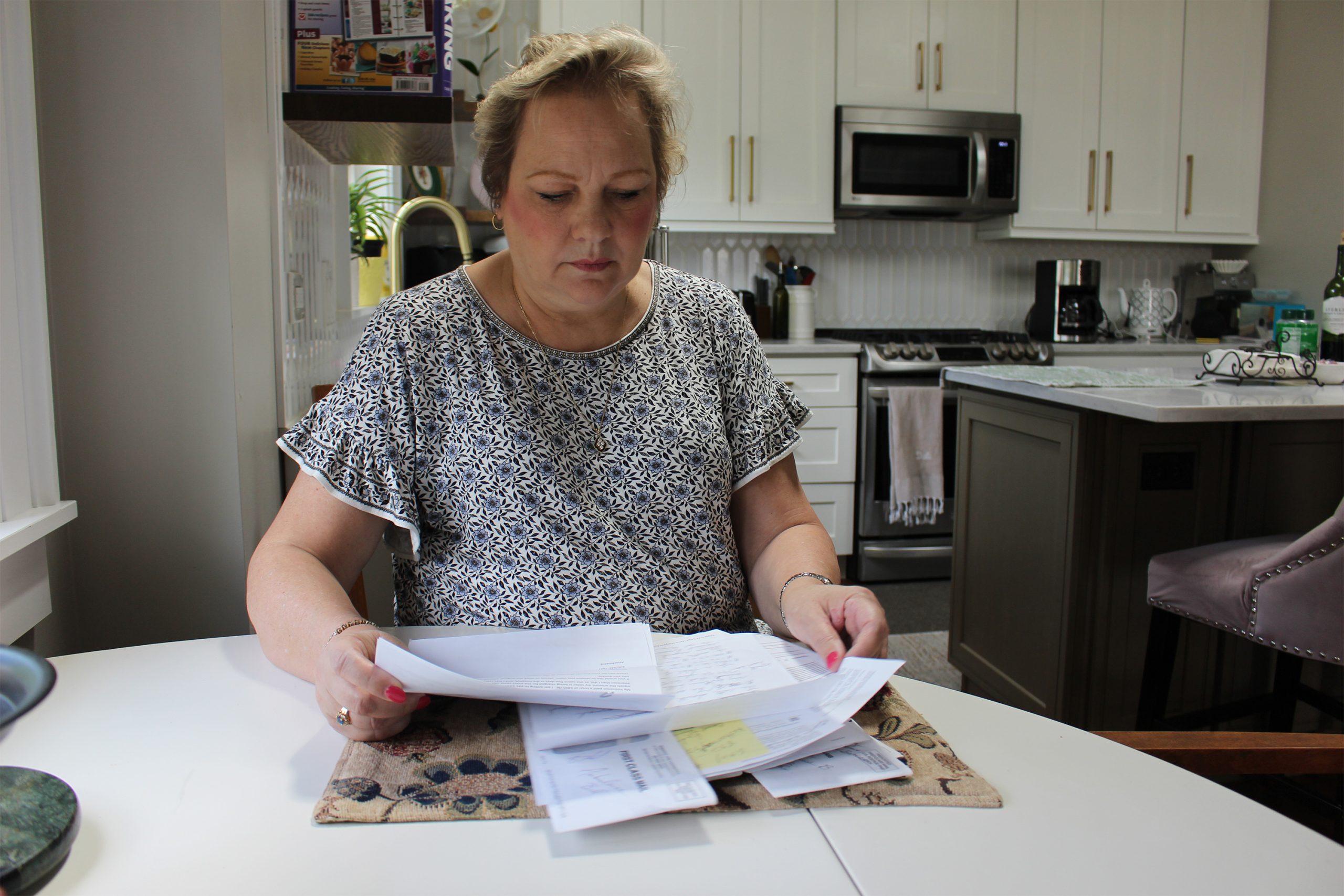
Bisi Bennett was charged $550,124 after her son was in a neonatal intensive care unit for nearly two months — despite having insurance. In a recent interview, nearly three years after her bill was investigated by “Bill of the Month,” she said she initially thought resolving the bill would be simple.

“Nine months later, 10 months later, I was still fighting with them,” she said. “I really did feel like it kind of robbed me a little bit of the joy of the first months of motherhood.”
Once a reporter started making calls, Bennett said, “they somehow miraculously figured out how to bill the right parties and get it sorted out.”
But relief from individual bills is one thing; patients say bigger solutions are needed for what ails our health system. “This isn’t just about my bill,” Calver said in 2018, when his nearly $109,000 bill was reduced to $332 after being investigated by “Bill of the Month.” “I don’t feel any consumer should have to go through this.”
The Takeaways
The “Bill of the Month” mantra is: If the bill is unexpected or seems off, don’t write the check. Each installment offered directions to navigate health care’s rough financial waters.
Some bills memorably illustrated the absurdity of a system that turns ordinary mishaps into extraordinary revenues. After 3-year-old Lucy Branson got a Polly Pocket doll shoe stuck up her nose, her family was charged about $2,659 for an ER doctor to fish it out with forceps — essentially a long pair of tweezers.
Here are some of the most important lessons — and some patients who offered their experiences to teach them:
- Before scheduling services, ask if a provider is in-network — then read waiting-room forms closely. Feeling sick and unable to rule out covid-19, Elyse Greenblatt booked a telemedicine appointment. But her in-network doctor’s office paired her with an out-of-network doctor — and said she’d signed a consent form. Her insurer declined to pay a penny of the $660 bill.
- Ask for an itemized bill, and question charges that don’t make sense. Eloise Reynolds paid her husband’s final hospital bill after he died from colon cancer. A year later, she received a second bill for his stay. Reynolds requested an itemized bill — and using a yardstick as a straight edge, went line by line to sort out why the hospital said she owed nearly $1,100 more. The balance was eventually deemed a “clerical error” and eliminated.
- Beware ambulances. The landmark No Surprises Act protected patients from many surprise bills in emergencies, but it does not apply to ground ambulances, which are unlikely to contract with insurance and thus might bill willy-nilly. When Peggy Dula was in a car accident, she was picked up by a fire department ambulance that was out-of-network. Though she wasn’t terribly hurt, her ride generated a $3,606 charge, and — after her insurance paid an amount it deemed “reasonable and customary” — she owed around $2,711.
- Location Matters, Part 1: Any intervention or test done in a hospital is likely to cost more than elsewhere. After her first prenatal checkup, Reesha Ahmed had her blood drawn for routine tests by a hospital lab. The bill: $9,520. Ahmed, who had a miscarriage, owed $2,390.
- Location Matters, Part 2: Doctors’ offices can be reclassified as hospital facilities if they’re purchased by a hospital system — and then add on hospital facility fees. Kyunghee Lee, a retired seamstress, went to her doctor for regular injections to treat arthritis for a copay of about $30. Then the office moved one floor up — and her bill changed: Newly designated as taking place in “a hospital-based setting,” one visit was billed at $1,394, including a facility fee listed as “operating room services.” Lee owed about $355.
- Location Matters, Part 3: Some free-standing emergency rooms may look like urgent care centers but come with ER charges. Tieqiao Zhang believed he was visiting urgent care when he sought treatment for a kidney stone at a facility called an “urgent care emergency center.” He went there twice and, both times, was given IV hydration and painkillers, then sent home. The visits yielded a bill of $19,543, including a $500 copay for each visit to what was actually a free-standing ER.
- Sometimes it can pay to pay cash. Dani Yuengling needed a breast biopsy after a concerning mammogram. The hospital’s online price calculator listed a price of about $1,400 for those without insurance. So she was shocked to see her own bill, paid using insurance, was almost $18,000, of which she owed more than $5,000 under the terms of her high-deductible plan.




The Resolution
Some bills signal that there’s more to be done to tame a health care industry in which seemingly everything can be billable. Mansi Bhatt took her toddler, Martand, to the emergency room for a burn on his hand, but after a long wait, they left before being seen by a doctor. Just checking in yielded an $859 bill, which the family had to pay since they hadn’t met their deductible.
Even new protections, such as those for air-ambulance bills, have problems. Amari Vaca was 3 months old and recovering from open-heart surgery when he contracted the life-threatening virus RSV, or respiratory syncytial virus. When doctors said he needed specialized care, he was transferred by air ambulance to a different hospital. The family’s insurer denied the claim, determining the flight wasn’t medically necessary, and the hospital declined to file an appeal. Vaca’s mother, Sara England, notified KFF Health News in October that their final appeal was denied. They owe $97,000.
And old bills die hard. When “Bill of the Month” reconnected with Phil Gaimon this fall, he said he had called his providers recently to check his outstanding balance — and learned it was, at last, zero.

Gaimon was competing to qualify for the Olympics when he was in a bicycle crash and wound up with bills topping $200,000. “I think I was home from the hospital in 10 days, riding my bike again in a month,” he said in an interview. “And then the bills … three years.”
While our “Bill of the Month” partnership with NPR is sunsetting, the “Bill of the Month” series will continue as KFF Health News investigates your medical bills. Keep them coming! And watch for future stories in The Washington Post’s Well+Being.
Elisabeth Rosenthal is a senior contributing editor for KFF Health News and the creator of “Bill of the Month.”
Emily Siner reported the audio story.
Henry Larweh and Molly Castle Work of KFF Health News contributed reporting for this article.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).

New Alberta COVID data highlights value of getting newly formulated vaccine once available: expert
The latest data published on the Alberta respiratory virus dashboard show that between August 2023 and August 2024, 732 deaths in Alberta were attributed to COVID-19.
Coronavirus
Your ‘summer cold’ could likely be COVID-19, doctors say amid surge
Gayle Robin was surprised when her sister in California told her in early July she had tested positive for COVID-19, which is rising in Canada, health experts say.
Coronavirus
Not too late to get flu, COVID-19 shots before Christmas: experts
With a record number of influenza cases recorded in Alberta, experts are recommending people get their flu shots.
Coronavirus
Quebec health-care establishments argue against allowing COVID-19 class action
If the case is allowed to go ahead, it would cover all residents of long-term care homes where COVID-19 outbreaks occurred during the first two waves of the pandemic.
Coronavirus
Manitoba’s two major political parties say they would not repeat COVID-19 lockdowns
Manitobans were never locked in their homes. But at the height of the pandemic, there were temporary restrictions on having visitors.
Coronavirus